
Healthcare content does not tolerate ambiguity. A patient instruction sheet, a medication guide, an informed consent form — these documents carry clinical weight, and when they cross language barriers, the risk does not disappear. It shifts into the hands of the translation method a hospital, clinic, or health information provider chose to use.
Language barriers in patient care remain one of the most underestimated contributors to medical error. Research consistently links miscommunication in clinical settings to adverse outcomes — from wrong medication dosages to misunderstood discharge instructions. As multilingual patient populations grow and healthcare organizations expand internationally, the question of how to translate content safely has become unavoidable.
This comparison breaks down the four most commonly used approaches, examines where each one fails, and identifies the conditions under which each is appropriate for healthcare-specific content.
Why Translation Accuracy Is a Patient Safety Issue
Medical errors already represent one of the most significant public health concerns in the United States. Approximately 400,000 hospitalized patients experience some form of preventable harm each year, with total costs to the healthcare system estimated in the tens of billions annually.
Translation failures contribute a measurable share of those errors. A 2025 industry analysis found that patients with limited English proficiency are 24 percent more likely to experience a clinical error than those who speak the primary language of the facility. The downstream effects include delayed diagnoses, incorrect medication use, non-compliance with post-care instructions, and avoidable readmissions.
The importance of accuracy in healthcare documentation applies equally to translated materials. The question is not whether to translate — it is which method produces output that clinicians, patients, and regulatory bodies can trust.
The Four Methods: A Side-by-Side Breakdown
Healthcare translation falls into one of four categories. Each has a distinct risk profile depending on document type, urgency, volume, and regulatory context. The table below summarizes the key operational and clinical trade-offs:
| Method | Best For | Accuracy | Speed | Cost | Compliance | Scalability |
|---|---|---|---|---|---|---|
| Certified Human Translation | Consent forms, drug labels, regulatory filings | ★★★★★ | ★☆☆☆☆ | $$$$$ | Full Section 1557 | ★☆☆☆☆ |
| Single-Engine Machine Translation | Quick internal reference only | ★★☆☆☆ | ★★★★★ | $ | Not recommended | ★★★★★ |
| MTPE (Human Post-Edit) | Discharge instructions, clinical documentation | ★★★★☆ | ★★★☆☆ | $$$ | With qualified review | ★★★☆☆ |
| Multi-Model Consensus AI | Health articles, admin content, high-volume outputs | ★★★★☆ | ★★★★★ | $$ | For non-critical docs | ★★★★★ |
Table 1: Comparison of healthcare translation methods across six criteria
Infographic: Visual Scorecard
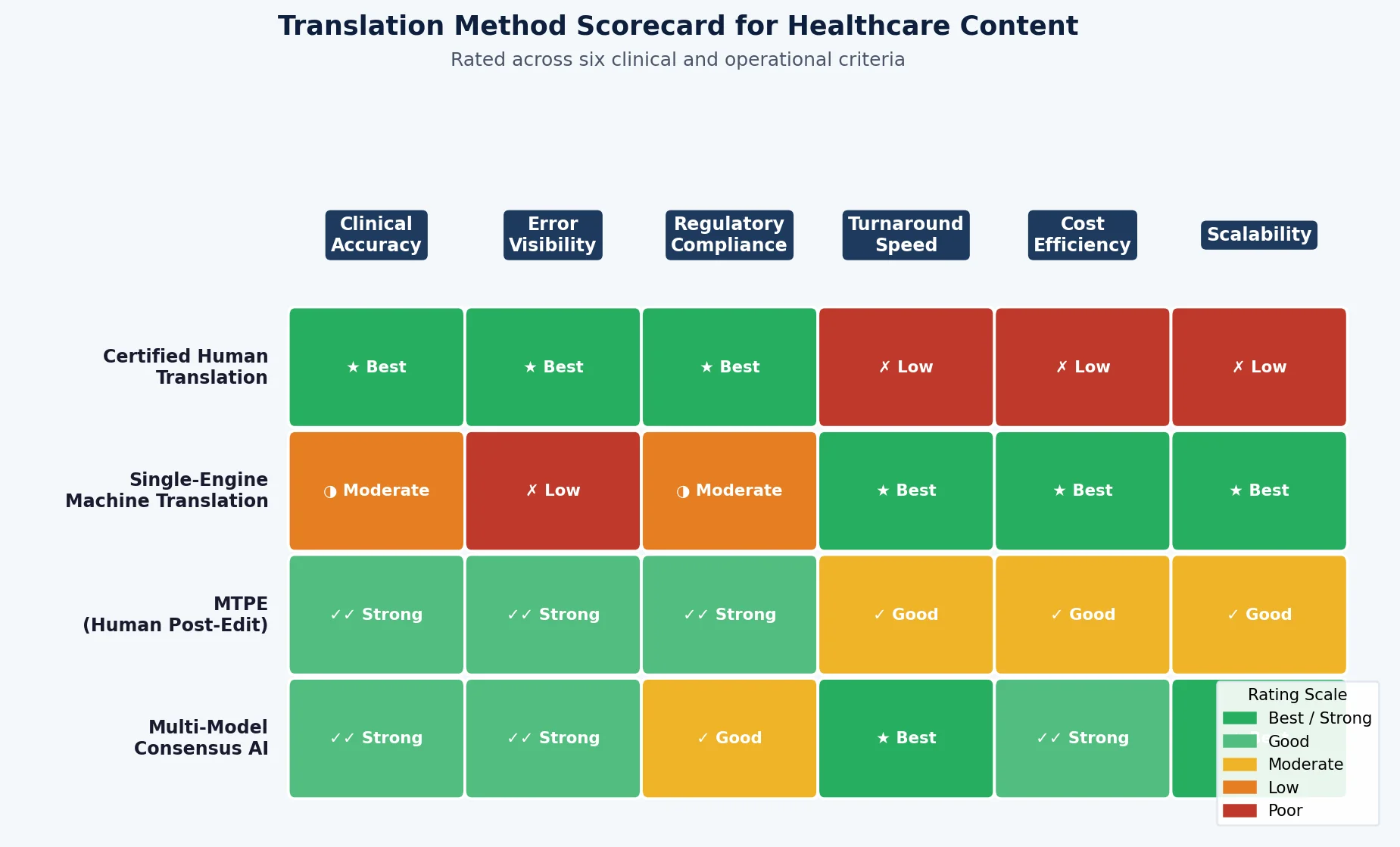
Figure 1: Translation Method Scorecard — Rated across six clinical and operational criteria
1. Certified Human Translation
Certified medical translators bring both linguistic competence and clinical domain knowledge. They can interpret terminology, recognize culturally loaded phrasing, and apply regulatory standards. For high-stakes documents — consent forms, drug labels, clinical trial protocols, patient safety notices — certified human translation remains the recognized gold standard.
- Strengths: Highest accuracy for complex clinical terminology; cultural adaptation; legal defensibility; Section 1557 compliance.
- Limitations: Cost, turnaround time, and scalability. Cannot keep pace with large-volume or time-sensitive content.
2. Single-Engine Machine Translation
Tools like a single-engine consumer translator offer speed and zero cost. Research published in 2025 confirms they remain the most commonly used translation tools in clinical settings despite not being purpose-built for medical use.
- Strengths: Immediate output; free or low-cost; no setup required.
- Limitations: No internal quality signal. A mistranslation appears with the same confidence as a correct output. Research on pediatric discharge instructions found clinically impactful errors across multiple language pairs — invisible in the output.
3. Machine Translation with Post-Editing (MTPE)
MTPE pairs AI speed with human review. A translator — ideally with clinical expertise — reviews machine output and corrects errors before publication. This reduces cost compared to full human translation while adding a quality layer that raw machine output lacks.
- Strengths: Faster and more affordable than pure human translation; human review catches clinical errors before they reach patients.
- Limitations: Quality depends heavily on the machine output fed to the reviewer. Subtle errors in the base translation increase reviewer burden and error risk.
4. Multi-Model Consensus AI Translation
A newer category that runs source content through multiple AI translation models simultaneously and applies a consensus mechanism to identify the most accurate output. Rather than producing one translation and calling it complete, multi-model systems compare outputs across engines, detect divergence, and surface the translation with the strongest cross-model agreement.
- Strengths: The consensus step provides an internal quality signal that single-engine tools lack. Speed and scalability maintained. Ideal for high-volume non-critical health content.
- Limitations: Does not replace human review for highest-stakes regulatory documents. Represents a meaningfully stronger automated baseline — not a substitute for certified translation where regulations require it.
Risk vs. Speed: Where Each Method Sits
The core trade-off in healthcare translation is not simply accuracy vs. cost. It is patient safety risk vs. operational speed. The chart below positions each method across both dimensions, with bubble size representing relative cost:
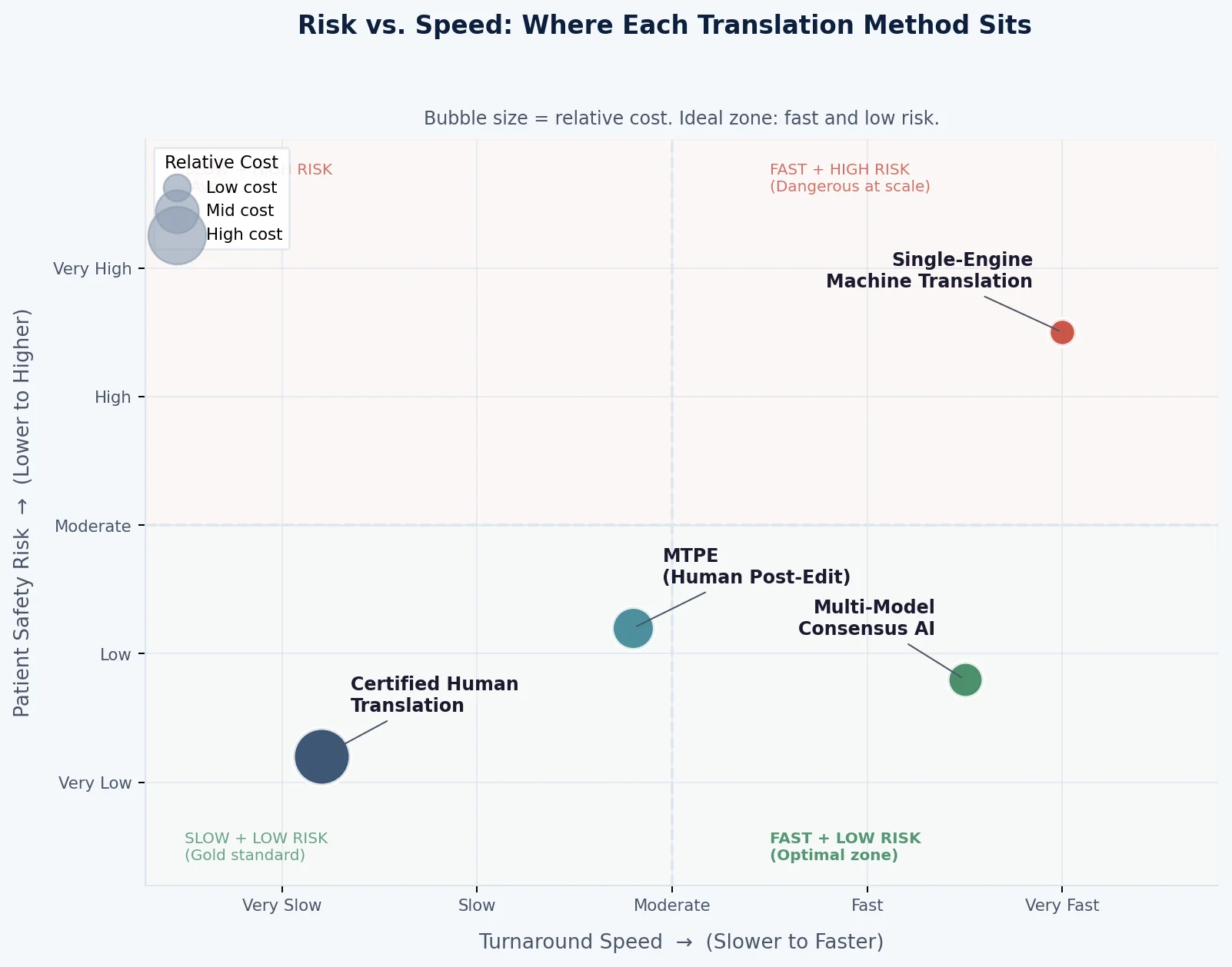
Figure 2: Risk vs. Speed positioning of four translation methods. Ideal zone: fast and low risk.
The Error Visibility Gap: Why Single-Engine Tools Fail Healthcare
The core weakness of any single-engine machine translation tool is not its average accuracy — it is its failure mode. Single-engine systems have no internal check. When they produce an error, it is delivered with the same presentation as a correct output. There is no divergence signal, no quality flag, no mechanism by which the system communicates uncertainty.
In healthcare content, this is particularly consequential. A translation of a medication instruction that appears correct but inverts a dosage, negates a contraindication, or uses a culturally familiar term carrying a different clinical meaning creates a patient safety risk that is invisible until harm occurs.
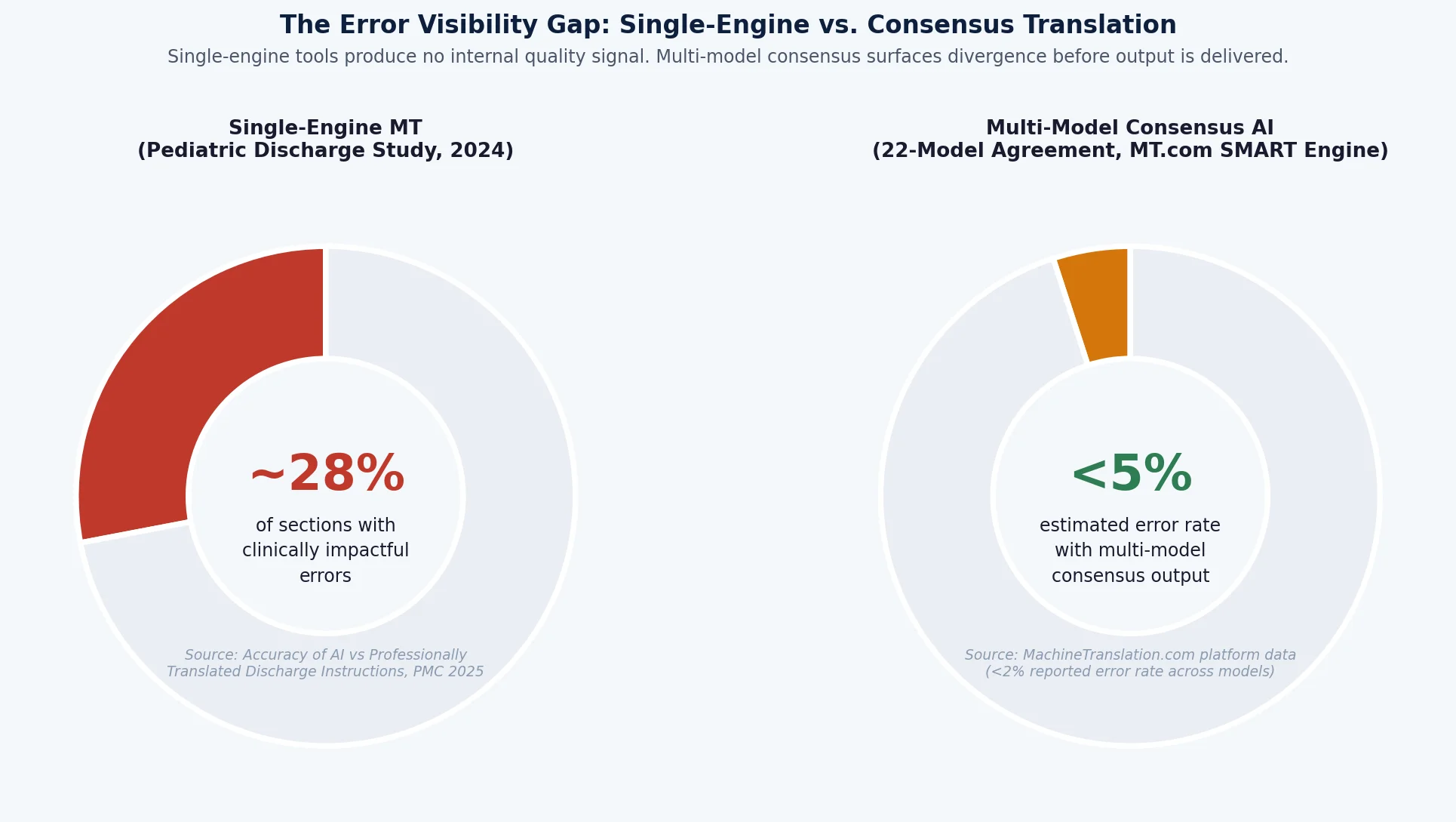
Figure 3: Error visibility gap between single-engine MT and multi-model consensus output
Multi-model consensus translation addresses this directly. Instead of asking one AI system to produce a translation and trust it, consensus-based tools run content through multiple models and analyze where they agree and where they diverge.
The Consensus Advantage: Why More Than One Model Matters
MachineTranslation.com operates on this principle. This AI translator developed by Tomedes, runs content through 22 AI translation models simultaneously, applying a SMART consensus engine to identify the highest-agreement output. For healthcare organizations translating patient-facing content at scale — health information articles, appointment reminders, educational materials, non-clinical administrative documents — this approach provides a meaningfully stronger automated baseline than any single-engine tool.
The practical benefit is not just accuracy. It is operability. Clinical teams using a consensus-based tool receive output with a higher inherent quality floor, reducing the burden on post-editors and reviewers. When human review is still required — for consent forms, drug labels, or regulatory submissions — reviewers are working from a stronger starting point.
For health content publishers, hospital communication teams, and digital health platforms managing multilingual content at volume, the distinction between single-engine and multi-model output is not theoretical. It is the difference between catching a clinical error at the source and delivering it to a patient.
Which Method for Which Document?
Not every healthcare document carries the same regulatory and clinical weight. The right translation method depends on the document type. The chart below maps suitability across the most common content types:
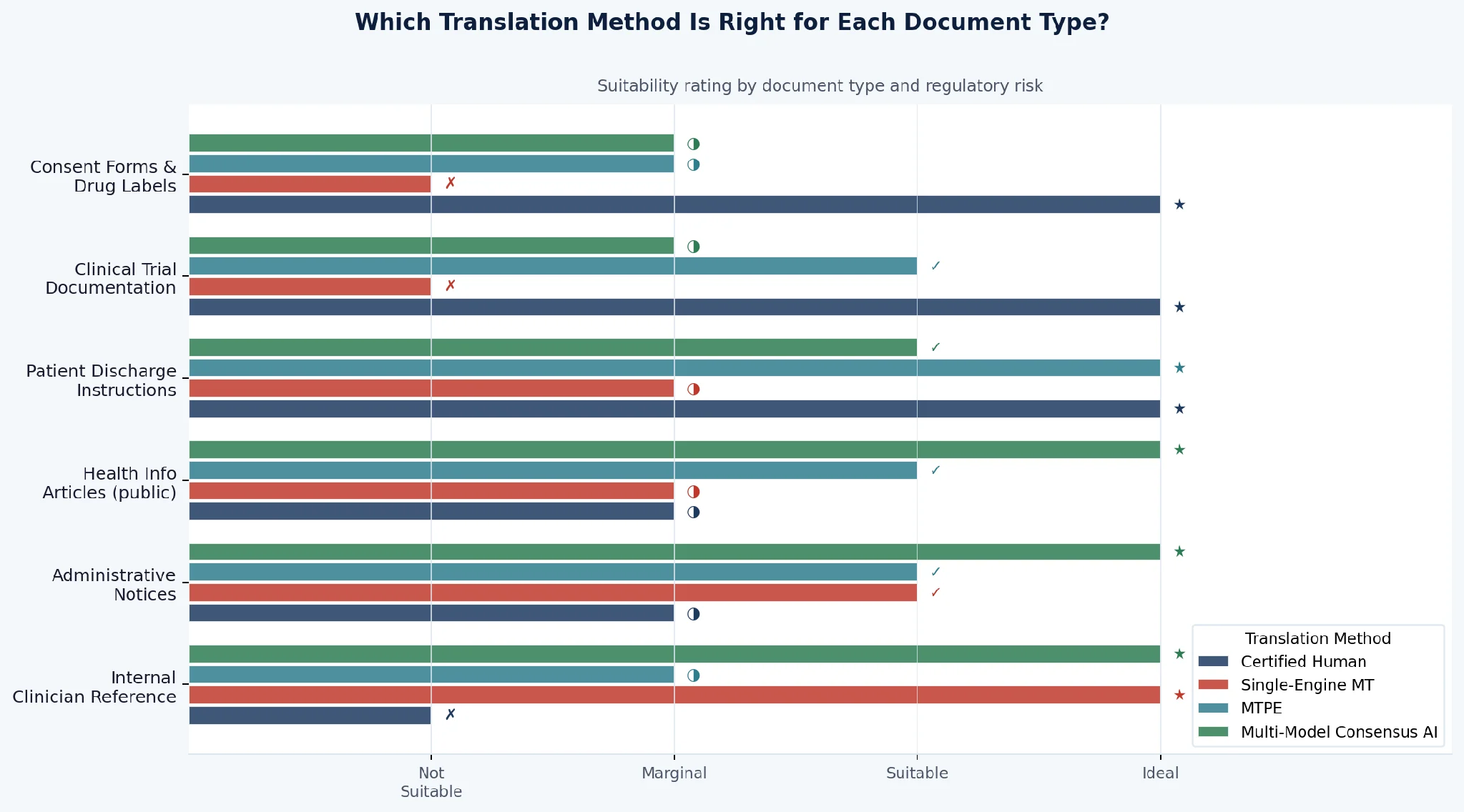
Figure 4: Suitability of each translation method by healthcare document type
Regulatory Considerations in 2026
Regulatory frameworks are beginning to catch up with the operational realities of AI translation in healthcare operations. The 2024 HHS Final Rule implementing Section 1557 provided the first explicit federal guidance on machine translation in clinical settings. It introduced a critical distinction between critical and non-critical documents. For critical documents — consent forms, discharge instructions, notices of eligibility — the regulation requires that a qualified human translator review and correct machine-generated content before it reaches a patient.
This creates what researchers describe as a regulatory human-in-the-loop floor for high-stakes clinical communication. For non-critical content — the majority of health information, educational materials, and operational communications — organizations have more operational flexibility, but the clinical stakes of error remain.
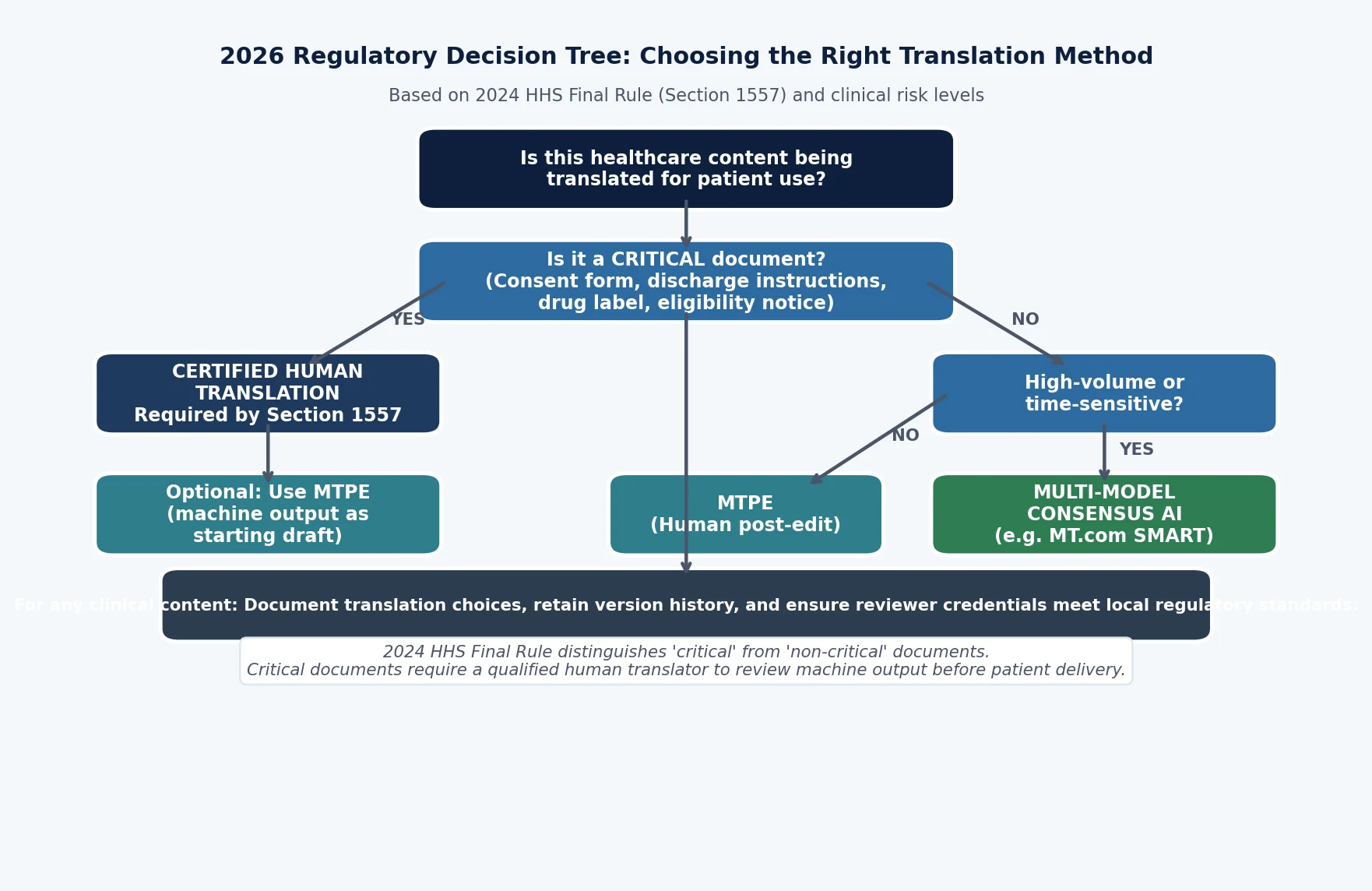
Figure 5: 2026 Regulatory Decision Tree for choosing the right translation method under Section 1557
Which Method Is Safest? A Framework
There is no single answer — because the answer depends on document type, regulatory requirements, volume, and available resources. But there is a framework:
- Regulatory and consent documents: Certified human translation with or without MTPE. Non-negotiable for Section 1557 compliance.
- High-volume non-critical content: Multi-model consensus translation provides the strongest automated baseline, with human review applied selectively to flagged or high-sensitivity content.
- Operational speed with oversight available: MTPE using consensus-based machine output as the starting point reduces post-editor workload and error rate simultaneously.
- Single-engine consumer tools: Appropriate only for informal internal reference — never for patient-facing content where errors carry clinical or regulatory consequences.
The architecture of translation matters as much as the act of translating. For healthcare organizations taking multilingual patient communication seriously, understanding the difference between a tool that produces one output and one that compares twenty-two is not a technical detail. It is a patient safety decision.